Abstract
Leber hereditary optic neuropathy (LHON) is a genetic disorder caused due to variations in the mitochondrial genome. Individuals with this condition present in the second/third decade with progressive central painless vision loss. Common pathogenic variants, m.3460G>A in MT-ND1, and m.11778G>A, and m.14484T>C in MT-ND6, are reported in around 95% of patients. Multiple studies with descriptions of phenotype, molecular basis, and prognosis are reported, however, only a few studies illustrate the importance of genetic counselling. This is a retrospective study. Here we aim to address and describe the challenges faced in the process of genetic counselling of two patients diagnosed with LHON and explain how these could be overcome. We highlight the importance of information on genotype-phenotype correlation, and cascade-screening in LHON and elaborate on the significance of psychosocial counselling.
Keywords: Leber hereditary optic neuropathy, reduced penetrance, cascade screening, genotype-phenotype correlation, genetic counselling.
Introduction
Leber hereditary optic neuropathy (LHON) is a mitochondrial disorder where affected individuals present in the second/third decade of life with progressive painless central vision loss (Yu-Wai-Man & Chinnery, 2000). The diagnosis of LHON is established by mitochondrial DNA sequencing. Around 95% of individuals diagnosed with LHON are observed to carry one of the three common variations including m.11778G>A and m.14484T>C in MT-ND6 or m.3460G>A in MT-ND1 (Yu-Wai-Man & Chinnery, 2000). Reduced penetrance can be observed in this condition which is the result of mitochondrial mutation load and its interaction with environmental factors. Additionally, it is also sex and age dependent. Penetrance in males is reported to be as high as 50-60% whereas in females it is 10-20% (Puomila et al., 2007). Further, the peak of onset of symptoms is in the second/third decade of life and the chances of developing vision impairment reduce drastically thereafter (Yu-Wai-Man & Chinnery, 2000). The prognosis of the condition has also been reported to depend on the type of variation causative of LHON, that is, the individuals harbouring the m.14484T>C variant are observed to have a better visual prognosis with a partial recovery rate of 37-58% (Theodorou-Kanakari et al., 2018). LHON is one of the first mitochondrial conditions for which approved treatment is currently available. In 2011, a randomized placebo-controlled trial showed that treatment through Idebenone had significant improvements in visual acuity in patients with LHON (Klopstock et al., 2011). Idebenone was approved in 2015 by the European Medical Agency for the treatment of LHON (Carelli et al., 2017).
Here, we aim to address and describe the challenges faced in the process of genetic counselling with the help of illustrative clinical scenarios of two patients who were diagnosed to have LHON and how these could be overcome.
Clinical Scenarios
Patient 1
A 37-year-old male individual [Proband 1 (Figure 1; II.2)], first-born of a non-consanguineous couple was referred to the genetics clinic by an ophthalmologist. He presented with complaints of progressively diminishing, painless central vision loss. He started noticing these symptoms in the last two years, with an intermittent blurring of vision. His peripheral vision is comparatively preserved. There is no significant family history. His medical records were reviewed. The visual evoked potential testing showed mildly prolonged P100 latencies on the right side. Magnetic resonance imaging (MRI) of the brain and orbits were normal. Fundus examination reported bilateral peripapillary telangiectasias. Genetic testing by mitochondrial genome sequencing was already performed for him, which revealed the presence of the m.14484T>C variant in MT-ND6, confirming the diagnosis of LHON.
The proband came for a genetic counselling session as he was unable to decipher the significance and long-term implications of his diagnosis. He is a ground engineer at the aviation services department and was anxious about losing his job as a result of the disease diagnosis.

Figure 1: Three-generation pedigree showing Proband 1 at II.2
Patient 2
A 30-year-old female [Proband 2 (Figure 2; II.2)], first-born to a non-consanguineous couple was referred to the genetics clinic by her gynaecologist. She presented with a history of visual impairment in herself and other family members. She first noted the onset of symptoms at 15 years of age with a mild blurring of peripheral vision, the symptoms progressed over the years and currently, there is a complete loss of vision. Upon taking a detailed family history, the proband revealed that her younger sister (in Figure 2; II.3) and brother (in Figure 2; II.4) also had similar complaints and currently both of them have blurred peripheral vision and no central vision. Proband’s mother (in Figure 2.; I.2) had complaints of central vision blurring, onset in the third decade of life, and the symptoms progressed after the birth of her youngest offspring. Currently, she has diminished central vision with preserved peripheral vision. MRI (brain and orbit) of the proband was suggestive of thinned-out optic nerves (right>left). Genetic testing by mitochondrial genome sequencing was ordered by her ophthalmologist which revealed the presence of m.11778G>A in MT-ND6, confirming the diagnosis of LHON.
The proband is a primigravida (gestational age of 23 weeks) and wanted to understand the risk of occurrence of a similar condition in her ongoing pregnancy.
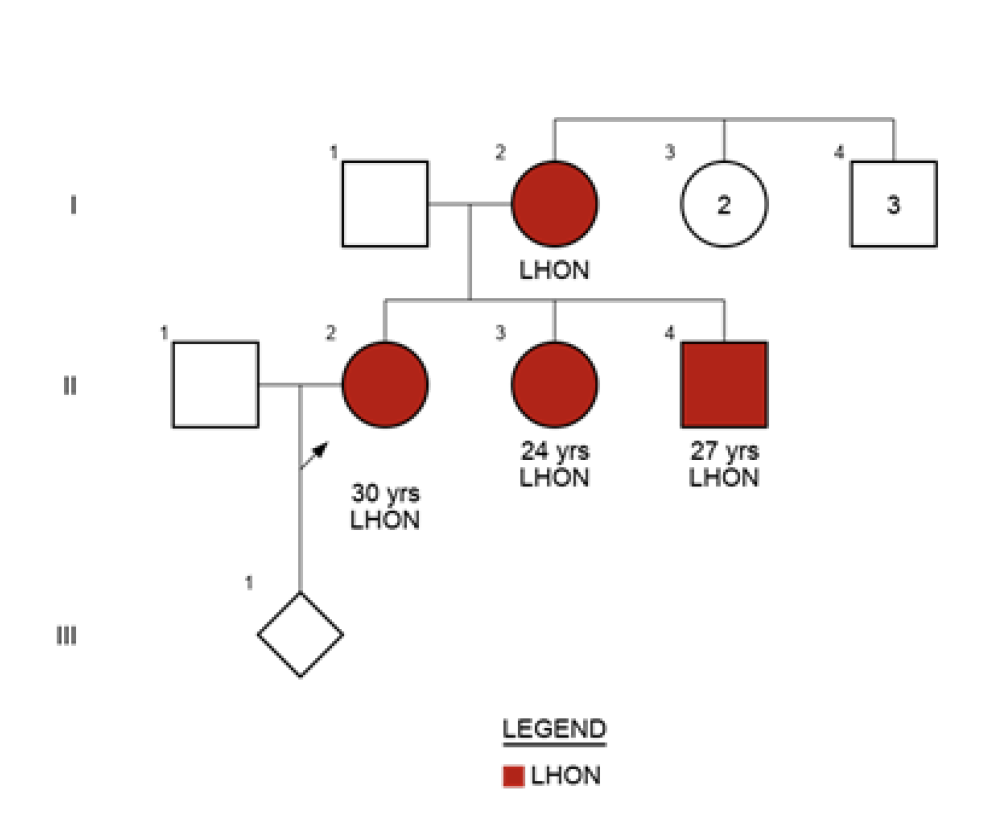
Figure 2: Three-generation pedigree with Proband 2 at II.2., her affected siblings at II.3., II.4., and affected mother at I.2.
Discussion
Innumerable complexities of mitochondrial genetics contribute to challenges faced during genetic counselling of individuals with LHON as well as for the family members who want to understand the risk of occurrence of a similar condition. Some of these features include:
1. Progressive nature of vision loss
2. Adult/adolescent onset of the condition
3. Maternal inheritance
4. Sex and age-dependent penetrance
5. Discrepancies in the practice of the prenatal diagnosis
Taking the above two family case scenarios, we discuss the specific challenges faced during the post-test genetic counselling session.
Genetic counselling in India
Specialist facilities of clinical geneticists and genetic counsellors are still not available in every hospital and people still have to travel to tertiary care centres to access these services. Thereby, genetic counselling services are mostly provided by either non-genetic medical practitioners or other health professionals with training in genetics.
With the increasing affordability and availability of genetic testing in India, physicians can now order a genetic test, and this is mostly without appropriate genetic counselling. A similar situation was faced in the above two families, where the genetic testing was advised without pre-test genetic counselling due to the non-availability of genetic counsellors in the hospital. The missed pre-test counselling sessions left the patients clueless about the expected results and implications of the disorder at hand. This challenge is observed within other specialties, for instance, neurology, cardiology, oncology, etc.
Presymptomatic genetic testing is performed for asymptomatic individuals with a family history of an adult / late childhood onset autosomal dominant disorder. The a priori risk of disease is usually 50% based on the pedigree. Targeted testing of the familial pathogenic variant is performed after appropriate genetic counselling. The test, performed before the onset of symptoms, requires counselling by an experienced geneticist, ophthalmologist and genetic counsellor. For a mitochondrial disorder such as LHON, there are unique challenges related to presymptomatic testing. A pathogenic variant in an asymptomatic individual is not predictive of disease. Specific LHON-causing pathogenic variants have variable penetrance based on the sex of the patient. The risk of developing the disease, the extent of the phenotypic manifestations and disease progression are specific for the mutation.It is imperative to refer to published data for the specific familial variant for presymptomatic genetic counselling ((Yu-Wai-Man & Chinnery, 2000).
Financial and economic insecurities in progressive disabling conditions
Non-lethal adult/adolescent genetic conditions can leave patients with life-modifying disabilities. LHON is a progressive condition that can lead to permanent visual impairment (Yu-Wai-Man & Chinnery, 2000). Although the prognosis of individuals with m.14484T>C in MT-ND6 is better, with better visual acuity, other variations of this condition can have a poor prognosis (Carelli et al., 2017).
Proband 1 who was a ground engineer at an airport, feared losing his job on receiving the diagnosis of LHON. He expressed his distress and worry with regards to the possible challenging financial situations as a sole earning member. Appropriate post-test genetic counselling and guidance of alternative employment options enabled him to communicate to his employer for reinstating him from a ground job to a desk job. Proband 2 was a homemaker and did not express concerns related to financial/economic insecurity.
Occurrence and recurrence in mitochondrial inheritance
Mitochondrial disorders pose challenges in reproductive counselling which includes explaining the occurrence and risk of recurrence of the disorder. In the process of providing information and educating, patients may end up feeling overwhelmed. Genetic counselling helped in conveying this information to the proband by using simple terms, visual aids, and appropriate counselling tools to simplify complex information that helped the affected person to understand and to effectively communicate the risks with other at-risk family members. Additionally, it facilitated informed decision-making and searching the reproductive options for subsequent pregnancies as in Proband 2.
Unavailability of condition-specific support groups
Awareness about genetic conditions is still emerging in developing countries like India. There are now well-established patient support groups and non-government organizations (NGOs) for a few common genetic conditions such as Down Syndrome, beta-thalassemia, fragile X syndrome, spinal muscular atrophy, etc. However, for rare conditions like LHON, unavailability still persists. This aggravates feelings of being lonely and helpless.
We were able to connect both the families to LHON-specific online support groups based in Canada and the United Kingdom. They were given information regarding patient groups on various social media platforms. Moreover, they were connected to a rare disease NGO in India that helped Proband 1 to receive Idebenone on a compassionate basis. Further, information regarding government policies for the visually impaired including employment transition, travel requirements, and allowances were provided.
Limitations of prenatal diagnosis for mitochondrial disorders
In case one, the proband (Proband 1) had completed his family. The mode of transmission of mitochondrial DNA is cytoplasmic. Since sperms do not transmit cytoplasm during fertilisation, there is no risk of transmitting the mitochondrial mutation and hence prenatal diagnosis is not indicated in this case if the couple plans a subsequent pregnancy in the future.
In case two, there was an ongoing pregnancy at the time of diagnosis confirmation. The pregnancy was advanced till diagnosis was made and the counselling was challenging for prenatal testing as the family was unaware of the limitations of prenatal diagnosis for LHON.
Homoplasmic mutations are reported to be the most common disease mechanism in LHON however, in 10-15% of cases heteroplasmy is also reported (Yu-Wai-Man & Chinnery, 2000). For instance, in a study, individuals with an m.11778G>A pathogenic variant load of less than 75% in their leukocytes were unaffected (Smith, 1993). Moreover, the penetrance of LHON is sex-dependent as discussed above but gender selection is a punishable felony in India under the Pre-conception & Pre-natal Diagnostics Techniques (PC-PNDT) act (Bhaktwani, 2012). Therefore, Proband 2 was told about various reproductive options she could consider such as egg donor or adoption for the subsequent pregnancies.
Further, the female sibling of the proband was advised genetic counselling regarding the risk of recurrence of the similar condition and to discuss reproductive options to avoid the same. The male sibling of the proband was explained the negligible risk of transmission of this condition in his offspring.
Mitochondrial replacement therapy with three parent babies is an option for a couple to prevent transmission of a mitochondrial mutation. The oocyte nucleus of the mother with mitochondrial disease and the enucleated oocyte of the donor with normal mitochondria is utilized for fertilization. This can be by male and female pronulear transfer from the at-risk zygote to the enucleated donor zygote. The second option is of maternal spindle transfer in metaphase II and transfer to the enucleated disease-free donor (Yu-Wai-Man & Chinnery, 2000).
Practices for improving lifestyle
Due to the progressive nature of the disease observed in Proband 1, a few lifestyle modifications were suggested to help him cope better with the condition. For instance, he was advised to avoid driving so as to prevent any mishappenings. As his current employment necessitates the use of a computer he was introduced to various online applications/websites and assistive technologies such as Zoom Text, Job Access with Speech which provides text magnification and voice-over settings. Additionally, he was advised to discontinue alcohol and tobacco consumption as this could exacerbate visual impairment.
Conclusion
In previous times, the information about genetic tests, their availability and high costs limited their uptake. In the present times genetic tests are commonly used by all clinicians in practice and this has posed major challenges to appropriate patient counselling. It is crucial to achieve genetic literacy, enhance awareness of relevance of pre and post-test genetic counselling and understand the need of appropriate training for care of patients with genetic disorders.
References
1. Yu-Wai-Man P, Chinnery PF. Leber Hereditary Optic Neuropathy. 2000 Oct 26 [Updated 2021 Mar 11]. In: Adam MP, Everman DB, Mirzaa GM, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK1174/?report=classic
2. Puomila A, et al. Epidemiology and penetrance of Leber hereditary optic neuropathy in Finland. Eur J Hum Genet. 2007; 15: 1079-1089.
3. Theodorou-Kanakari A, et al. Current and Emerging Treatment Modalities for Leber’s Hereditary Optic Neuropathy: A Review of the Literature. Adv Ther. 2018;35:1510-1518.
4. Klopstock T, et al. A randomized placebo-controlled trial of idebenone in Leber’s hereditary optic neuropathy. Brain. 2011; 134: 2677-2686.
5. Carelli V, et al. International Consensus Statement on the Clinical and Therapeutic Management of Leber Hereditary Optic Neuropathy. J Neuroophthalmol. 2017;37:371-381.
6. Smith KH, et al. Heteroplasmy in Leber’s hereditary optic neuropathy. Arch Ophthalmol. 1993;111:1486-1490.
7. Bhaktwani A. The PC-PNDT act in a nutshell. Indian J Radiol Imaging. 2012;22:133-134.