Carrier Screening in the Current Era: A Report Depicting its Utility and Challenges
Aashita Takkar, Veronica Arora, Swasti Pal, Renu Saxena Institute of Medical Genetics and Genomics, Sir Ganga Ram Hospital, New Delhi, India Correspondence to: Dr Veronica AroraEmail:veronicaarora@gmail.com
1 Abstract
Reproductive carrier screening is a genetic test which is offered to healthy individuals or couples who either have a history
of a previous child suspected with a genetic condition or are planning a pregnancy. It is carried out to identify
pathogenic/likely pathogenic variants in clinically relevant disease-causing genes known to be associated with autosomal
recessive or X-linked disorders. The updated carrier screening guidelines (2021) by the American College of
Medical Genetics and Genomics have introduced the concept of a tier-wise testing approach as this would be
essential for standardizing and making the test more cost-effective. Carrier screening helps in preventing the
recurrence of a known genetic condition and/or the birth of the first affected child with a genetic disorder.
We discuss a couple in whom carrier screening identified an autosomal recessive condition, ‘fetal akinesia
deformation sequence 2’. The test result helped to provide an answer for the couple’s bad obstetric history, a
risk estimate for the occurrence of this condition in their subsequent pregnancies and discussion of future
reproductive options. We also discuss the challenges and limitations of such testing and the ways to overcome
them.
Carrier screening is a type of genetic testing that is offered to asymptomatic couples as every individual is likely to be
carrier of variant/variants in one or more genes associated with autosomal recessive genetic conditions. Healthy
individuals are screened for heterozygous status of variants in genes that are associated with autosomal recessive and
X-linked recessive conditions of significant severity. It is ideally performed preconceptionally to identify couples who are at
risk of having a child with a monogenic disorder with significant clinical severity justifying the need for prenatal
diagnosis.
We describe a consanguineously married couple in whom carrier screening revealed them to be heterozygous carriers of
a likely pathogenic variant c.38G>T (p.Gly13Val) (Richards et al., 2015) in exon 1 of RAPSN, associated
with an autosomal recessive condition, fetal akinesia deformation sequence. The utility and challenges in
reproductive carrier screening are brought to light, emphasizing the value of correct interpretation of the
test.
3 Clinical Details
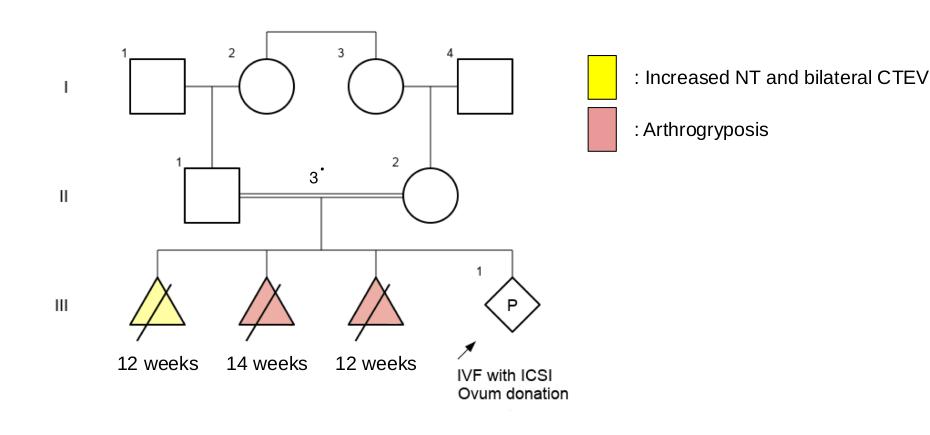
A third-degree consanguineously married couple (Figure 1) visited the genetics clinic in view of bad obstetric history.
Their first pregnancy was terminated for increased nuchal translucency (5.5 mm) and bilateral congenital equinovarus
deformity, at 12 weeks of gestation. No genetic testing or post-natal examination was performed on the fetus. Karyotypes
of the couple were normal. She conceived again after one year. The pregnancy was uneventful until 14 weeks, when
arthrogryposis was identified. Contractures were noted in bilateral elbow, knee, and ankle joints. This fetus also did not
undergo any genetic workup.
Figure 1: Three-generation pedigree showing two consecutive pregnancies affected with fetal akinesia deformation
sequence and a fourth ongoing pregnancy conceived with ovum donation.
The couple presented to the genetics clinic for preconception counseling and to understand the etiology in the previous
two fetuses as well as the risk of recurrence in their next pregnancy. In view of two previously affected pregnancies and
consanguinity, carrier screening was advised. High-performance liquid chromatography (HPLC) was also recommended to
check for beta-thalassemia trait status in the couple considering its high carrier frequency in the Indian population.
Pre-test genetic counseling was performed, and the couple opted to undergo Tier 3 carrier screening. The test was carried
out using next-generation sequencing (clinical exome sequencing). The results reported the presence of a
heterozygous variant of uncertain significance (VUS), c.38G>T (p.Gly13Val) (Richards et al., 2015) in
exon 1 of RAPSN in the couple, which is known to cause fetal akinesia syndrome as well as congenital
myasthenia syndrome type 11 in the biallelic state. The variant was reclassified as likely pathogenic after
genotype-phenotype correlation. Fulfilled criteria included PP4 (phenotype highly specific for the disease), PM2
(extremely low frequency in gnomAD population database), and PP3 (computational prediction tools support a
deleterious effect on the gene). Various in silico prediction tools like MutationTaster2 and SIFT reported the
variant to be damaging and Polyphen2 reported it to be probably damaging. HPLC showed normal levels of
HbA2.
As per the results of carrier screening, the couple was counseled for the risk of occurrence of this condition in their
subsequent pregnancies. Reproductive options were discussed. The options of prenatal diagnosis (PND) by chorionic villus
sampling (CVS) at 11 weeks and in vitro fertilization with preimplantation genetic testing-for monogenic disorders
(PGT-M) were explained in detail. An additional option of using a donor egg or sperm was also discussed. After extensive
counseling and discussion, the couple decided to plan their third pregnancy naturally followed by PND with
CVS.
The couple returned in their next pregnancy with the 12-week ultrasound suggestive of arthrogryposis multiplex. CVS
was performed followed by targeted variant analysis in RAPSN. The testing confirmed the affected status of the fetus and
the couple decided to discontinue the pregnancy (Figure 2). Subsequently, the couple was anxious and reluctant for
spontaneous conception. They decided to opt for in-vitro fertilization with ovum donation and intracytoplasmic sperm
injection (ICSI), in view of the high cost of PGT-M.
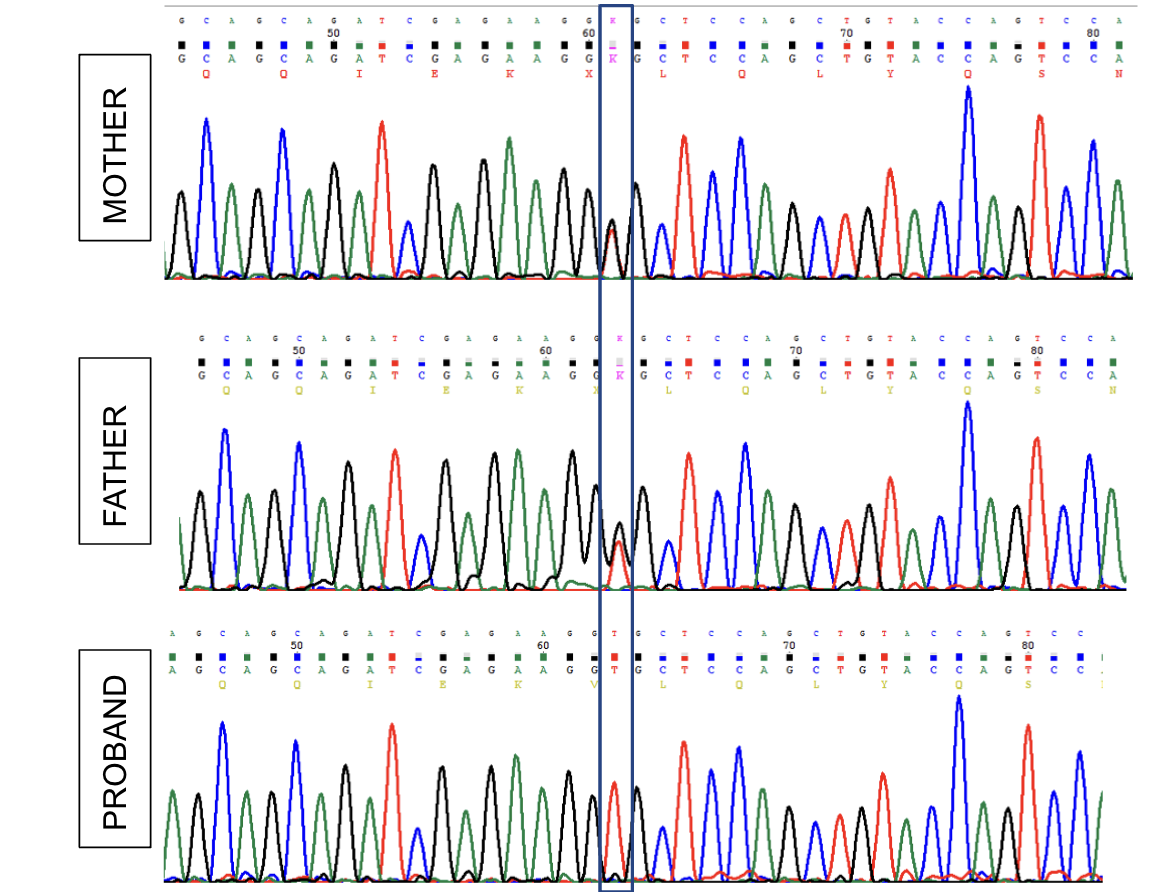
Figure 2: Sanger sequencing chromatograms demonstrate the c.38G>T (p.Gly13Val) variant in exon 1 of RAPSN
in heterozygous form in both partners and homozygous form in the affected fetus.
4 Discussion
Advances in the field of medical genetics and genomics have endowed us with a plethora of options for genetic testing that
not only provide a timely diagnosis of the condition but also help in preventing the occurrence/recurrence of a genetic
disorder in the family. In this family the variant in the gene which could explain the phenotypes of the
previously affected fetuses was identified. This option of identifying causative variants in the family in the
absence of sample of the proband is remarkable and very useful. However, it is necessary to create awareness
about storing blood or a piece of umbilical cord of terminated fetuses or of sick babies who are unlikely to
survive.
Carrier screening may be advised to healthy individuals (majorly, to couples planning pregnancy), for
consanguineously married couples, or who have had a family history or history of a previous child with
a suspected/known genetic condition. There are numerous advantages of performing carrier screening. Carrier
screening helps in understanding the reproductive risk, avoiding recurrence of a genetic condition when
there is a family history, preventing the birth of the first affected child and timely discussion of reproductive
options. From a public health point of view, carrier screening helps in decreasing financial as well as disease
burden in the country (Bajaj et al., 2014). Wilson and Junger, in 1986, established the criteria that guided
the selection of conditions for carrier screening. These criteria were later updated by the World Health
Organization in 2008 (Bajaj et al., 2014). In 2005, the American College of Obstetrics and Gynecology
(ACOG) and the American College of Medical Genetics and Genomics (ACMG) provided guidelines and
general recommendations for screening of different conditions as well as for the screening of population-specific
variants (Bajaj et al., 2014). Carrier screening was previously divided into targeted and expanded carrier
screening, where targeted screening was performed based on the specific ethnicity/ community. For instance,
screening was performed for disorders like Tay-Sachs disease, Canavan disease, cystic fibrosis, and familial
dysautonomia in Ashkenazi Jews. On the other hand, expanded carrier screening comprised next-generation
sequencing (NGS)-based testing for parallelly sequencing multiple genes associated with autosomal recessive
or X-linked recessive disorders. These terminologies are still frequently used. However, the updated 2021
ACMG carrier screening guidelines have recommended avoiding the usage of these terminologies as they are
less precise and hence, have established a tier-wise approach to screening (Gregg et al., 2021). According to the guidelines,
there are four tiers to the screening process. Tier 1 is to screen for cystic fibrosis and spinal muscular atrophy. Tier 4 aims
to look for pathogenic (P)/likely pathogenic (LP) variants for less common genetic disorders. Tier 4 testing is not usually
recommended until there is consanguinity, significant family history of the condition, or a history of a previous child with
a suspected/known genetic condition. The guidelines recommend that Tier 3 carrier testing which includes testing for
genetic conditions with a carrier frequency of >1/200 should be advised for all the couples who are planning a pregnancy.
Furthermore, extensive pre-test and post-test counseling should be carried out for the couples opting for carrier screening
especially in couples with no family history of a genetic disorder. (Gregg et al., 2021). Pre-test counseling should be
carried out to discuss the benefits, limitations, implications, costs and turn-around time, and help the couple to facilitate
informed decision making. During pre-test counseling, the possibility of detection of variants of unknown significance
should also be mentioned. Post-test counseling should be done to help the couple interpret the reports, discuss about
reproductive options if required and address the emotional consequences. The use of genome sequencing for preconception
carrier screening has been reported to improve the sensitivity of detecting clinically significant variants. However, the
interpretation of novel variants and variants of uncertain significance makes this not worth its while (Punj et al., 2018).
This is the major challenge of NGS-based carrier screening though the cost is also a concern for many families. The
detection of VUS poses a challenge and a need for expert analysis. Ideally, reporting of variants should be limited to
pathogenic and likely pathogenic variants. However, in instances where one of the partners is a carrier of an LP/P variant,
or in case of relevant family history, reporting a VUS is reasonable after analysis by an expert. It has been
documented that many causative variants in Indian patients are different from those reported worldwide and till
there is a big database of LP/ P variants from Indian population, many of the variants will continue to be
novel. Lastly, the field of medical/molecular genetics is constantly expanding, and the disease causation of
many genes/variants is still unknown or lacks evidence. Due to this, the undetermined information that
we might obtain with the current advancements could be significantly established in the future (Sparks,
2020).
The option of assisted reproductive technology, though a possibility in couples who are found to be carriers, has its
own cons, including a failure rate of as high as 40%, the difficulty in testing the embryos, and the cost. The interpretation
of the carrier screen reports could be challenging, especially in view of an overall small number of geneticists in the
country. But it is safe to say that uniform reporting guidelines across the country can make the interpretation easier.
Finally, it is never easy to counsel a patient and the family about the carrier status and the need for testing them, in the
absence of family history. The potential of carrier screening is huge, but a lot of hurdles need to be crossed before it can
be fully tapped.
References
1. Bajaj K, et al. Carrier screening: past, present, and future. J Clin Med. 2014; 3:1033-1042.
2. Gregg AR, et al. Screening for autosomal recessive and X-linked conditions during pregnancy and
preconception: a practice resource of the American College of Medical Genetics and Genomics (ACMG). Genet
Med. 2021; 23: 1793-1806.
3. Punj S, et al. Preconception Carrier Screening by Genome Sequencing: Results from the Clinical Laboratory.
Am J Hum Genet. 2018; 102: 1078-1089.
4. Richards S, et al. Standards and guidelines for the interpretation of sequence variants: a joint consensus
recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular
Pathology. Genet Med. 2015; 17: 405-424.