Silver-Russell Syndrome: Case Report and Insights for Prenatal Diagnosis
Seema Thakur1*, Preeti Palliwal2, Arpana Jain1, Tanu Gera1, Sunita Kapoor3, Deepa Khurana3 1Fortis Hospital, Shalimar Bagh, New Delhi, India 2Sir Ganga Ram Hospital, New Delhi, India 3City Xray and Clinic, New Delhi, India Correspondence to: Dr Seema ThakurEmail:seematranjan@gmail.com
1 Introduction
Silver–Russell syndrome (SRS), OMIM #180860, is characterised by prenatal and postnatal growth retardation. The
syndrome was initially described in a group of children with low birth weight, atypical facies, postnatal short stature and
body asymmetry independently by Silver et. al. (1953) and Russel (1954). The presentation of intrauterine growth
retardation and small for gestational age (SGA) is extremely heterogeneous, however SRS can be distinguished from those
with idiopathic intrauterine growth retardation or SGA and postnatal growth failure by the presence of several
characteristic features. An underlying genetic cause can be identified in around 60% of patients clinically diagnosed with
SRS (Netchine et al., 2007).
The present study reports a case of Silver-Russell syndrome that was identified on chromosomal microarray done after
intrauterine death. We have also reviewed the antenatal presentation of Silver-Russell syndrome.
2 Clinical findings
A 25 years-old primigravida was referred at 12 weeks of pregnancy in view of the first trimester combined screen showing
intermediate risk for Down syndrome (1 in 1204); low risks of 1 in 10,000 were noted for trisomy 13 and 18.
Pregnancy-associated plasma protein A (PAPP-A) was 0.57 MoM and beta human chorionic gonadotropin (βHCG) was
2.95 MoM. Her serum placental growth factor (PlGF) was 9 pgm/ml (0.20 MoM). First trimester NT (nuchal
translucency) scan showed NT of 1mm with crown-rump length (CRL) of 66.8mm and nasal bone measurement of 2.9
mm. Ductus venosus (DV) was normal and no tricuspid regurgitation was noted. The right and left uterine artery
pulsatility index (PI) were 2.57 and 1.97 respectively. The patient was not hypertensive and there was no history
of diabetes. Tab Ecosprin (150 mg aspirin) at bedtime was advised in view of the low serum PlGF and
increased uterine artery PI. NIPS (non-invasive prenatal screen) was offered in view of the intermediate risk for
aneuploidy. The results of NIPS showed low risk of aneuploidy for chromosomes 13, 18, 21 and sex chromosomes
with fetal fraction noted to be 4% for the test. Intrauterine demise (IUD) was detected at 17 weeks of
pregnancy and the fetus, along with placenta, was submitted for autopsy, low resolution microarray (315 K) and
histopathology.
2.1 Autopsy findings
Autopsy showed a male fetus with a foot length of 2 cm corresponding to 15 weeks gestation. The CRL was 10 cm, head
circumference (HC) was 11 cm and chest circumference was 9.5 cm, all of which corresponded to around 15 weeks
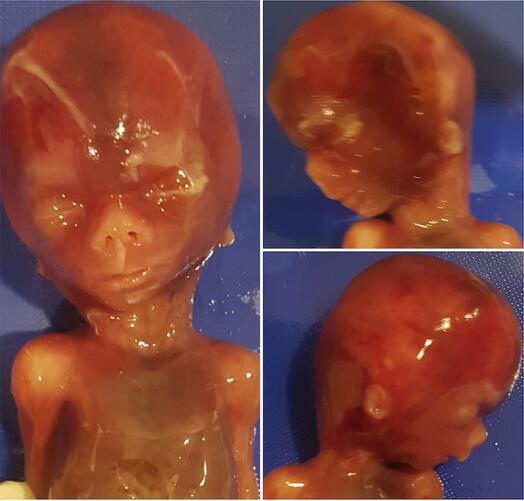
gestation. The external facial features noted were a triangular face, pointed chin, small nose, long philtrum, thin lips,
overhanging columella, low set ears and a prominent head (Figure 1). The upper limbs were noted to be reaching up to
the waist, indicating mildly short limbs.
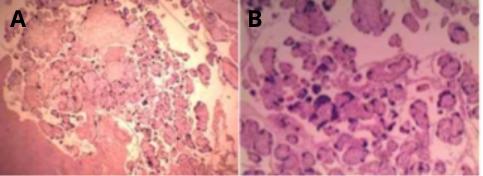
Placental histopathology suggested microinfarction of the placenta (Figure 2).
Figure 1: Craniofacial features of the fetus include a prominent head, triangular face, pointed chin, small nose,
long philtrum, thin lips, overhanging columella, and low set ears.
Figure 2: Histopathology of the placenta showing A. placental microinfarction & B. increased syncytial knots.
2.2 Genetic analysis
Chromosomal microarray analysis (CMA) was performed using the CytoScan Optima (315K) array (Affymetrix, Thermo
Fisher Scientific, USA) which showed a gain at cytoband 11p15.5p15.4 (1962499-2871270) encompassing
about 909 Kbps on chromosome 11. The microduplication on 11p15.5 overlaps with the 11p15.5-p15.4
microduplication syndrome. The important OMIM genes underlying the duplicated region are IGF2, KCNQ1, H19,CD81.
Methylation assay was performed for both IC1 (H19DR) and IC2 (KvDMR) loci and the results indicated
hypomethylation at the IC1 locus further confirming the diagnosis of SRS.
In view of a duplication, parental karyotyping was done to check for the presence of balanced translocation. Parental
karyotypes were normal. Parental microarray was not done.
3 Discussion
Silver-Russell syndrome is a rare syndrome characterised by low birth weight, short stature, craniofacial dysmorphism,
hemihypertropy and elevated urinary gonadotropins (Silver et al., 1953; Russell, 1954). Prenatal diagnosis of this
syndrome is not reported and the antenatal cases reported in literature actually had postnatal diagnosis based on
dysmorphic features and intrauterine growth restriction (IUGR). Wax et al. (1996) reported a fetus with asymmetric
IUGR which was diagnosed as Silver-Russell syndrome postnatally. Serial examinations at 23, 26, 27, and 29 weeks
showed continued head growth along the 10th centile and trunk growth along the 25th centile whereas the long bones
measured below the fifth centile for gestational age and also asymmetry in the long bones was observed. There were no
limb fractures, malformations, or deformations detected on ultrasound. Placenta was thick and histopathology showed
infarction.
Khalil et al. (2008) also reported a fetus with early onset IUGR first noted at 19 weeks 5 days, with abdominal
circumference less than 3rd centile. With advancing gestation, femur growth also declined to less than 3rd
centile, while the biparietal diameter (BPD) and HC were within normal limits. SRS was also reported in a
term baby of a 35 years old mother with head sparing IUGR (Johnson & Mokuolu, 2001). In this reported
fetus, intrauterine demise occurred at 17 weeks gestation, so serial growth parameters are unavailable.
But at this gestation BPD corresponded to 16 weeks, AC was at 15 weeks and FL at 14 weeks 4 days.
Histopathology of the placenta showed placental microinfarction. There was growth lag of about 1 to 2 weeks at the
time of IUD. Growth and amniotic fluid were normal in the first trimester NT scan. This is consistent
with other cases reported in literature, but IUD has not been reported in this syndrome earlier. This may
be due to associated uteroplacental insufficiency in our case. This may also be due to the fact that some
cases of fetal SRS may have been missed due to the lack of autopsy and microarray testing in cases with
IUD.
SRS is a genetically heterogeneous condition. Genetic testing confirms clinical diagnosis in approximately 60% cases
only (Netchine et al., 2007) Hypomethylation of the imprinting control region 1 (ICR1) at 11p15.5 is found in 35%-50% of
patients and maternal uniparental disomy of chromosome 7 is found in 7%-10%. There are some cases with SRS who have
duplications, deletions or translocations involving the imprinting centres at 11p15.5 or duplications, deletions, or
translocations involving chromosome 7. Rarely, affected individuals with pathogenic variants in CDKN1C, IGF2, PLAG1,
and HMGA2 have been described. In the reported fetus, chromosomal microarray showed a 909 Kbp duplication at
chromosome 11p15. Methylation testing at ICR1 suggested hypomethylation which confirmed the diagnosis of
Silver-Russell syndrome.
Majority of cases with SRS have been reported to occur sporadically and risk of recurrence in cases with methylation
abnormalities is low (Eggermann et al., 2016). In contrast, constitutional mutations (point mutations, duplications and
deletions) are associated with a significantly increased recurrence risk of up to 50% depending upon the gender of the
transmitting parent. The risk of recurrence for maternally inherited 11p15 duplication has been reported to be
as high as 50%. Also, it further warrants karyotyping of the parents to look for balanced translocation.
However, an important consideration that should be kept in mind while counselling the families when the
proband harbours a small sized duplication is that a normal karyotype does not rule out the possibility
of the mother being an asymptomatic carrier of the small duplication, because karyotyping has limited
resolution.
Fetal growth restriction (FGR) (fetal weight less than 3rd centile) is the key prenatal clinical feature of SRS but SRS is
usually not suspected antenatally as FGR is a common presentation and can occur due to various maternal, fetal or
placental causes. Fetal causes include genetic and epigenetic disorders or congenital fetal infections (Meler et
al., 2020). Prenatal diagnosis of SRS is usually done in the setting of a familial translocation involving
chromosome 7 or when mosaic trisomy 7 is detected in chorionic villus sampling. A knowledge of the postnatal
dysmorphic features of SRS will help in better identification of the fetal phenotype as for other genetic
syndromes.
The following points can provide important diagnostic clues for SRS in the antenatal period:
1. There is early onset growth restriction (before 32 weeks of gestation) after normal first trimester growth.
FGR can be mild to severe depending upon the severity of the case; variability in severity is seen postnatally
also.
2. Head circumference ≥1.5 SD above birth weight and/or length is one of the diagnostic criteria considered
postnatally. A large head compared to the limbs and abdominal circumference, is the most important clue
to suspect this syndrome in the antenatal ultrasound. (Meller et al., 2020)
3. Limb asymmetry is frequently noted in children with this syndrome and measurements of all long bones
(femur, tibia, fibula, humerus, radius and ulna) on both sides is therefore important.
4. 3 D examination of the face for features such as broad forehead and triangular chin may support the clinical
suspicion (Meller et al., 2020)
5. Examination of the genitalia for abnormalities such as hypospadias (Meller et al., 2020)
6. A normal Doppler ultrasound will support this diagnosis but at times uteroplacental insufficiency can be an
associated finding.
7. SNP microarray and methylation studies will confirm the diagnosis of SRS.
Since there are no clinical criteria for the diagnosis of SRS in a fetus, a keen eye to look for this condition will help families in
genetic counseling and in assessing the risk of recurrence in the subsequent pregnancies.
References
1. Eggermann T, et al. Prenatal molecular testing for Beckwith–Wiedemann and Silver–Russell syndromes: a
challenge for molecular analysis and genetic counseling. Eur J Hum Genet 2016; 24: 784–793.
2. Johnson AW, Mokuolu OA. Russell-Silver syndrome in a Nigerian infant with intrauterine growth
retardation. J Natl Med Assoc 2001; 93: 185–194.
3. Khalil H, et al. Russell–Silver syndrome presenting as early asymmetric IUGR. Ultrasound 2008;16: 87–90.
4. Meler E, et al. Genetic syndromes associated with isolated fetal growth restriction. Prenat Diagn 2020; 40:
432–446.
5. Netchine I, et al. 11p15 imprinting center region 1 loss of methylation is a common and specific cause
of typical Russell–Silver syndrome: clinical scoring system and epigenetic-phenotypic correlations. J Clin
Endocrinol Metab 2007; 92: 3148–3154.
6. Russell A. Syndrome of intrauterine dwarfism recognizable at birth with cranio-facial dysostosis,
disproportionately short arms, and other anomalies: five examples. Proc R Soc Med 1954; 47:1035–1044.
7. Silver HK, et al. Syndrome of congenital hemihypertrophy, shortness of stature, and elevated urinary
gonadotropins. Pediatrics 1953; 12: 368–376.
8. Wax JR, et al. Prenatal sonographic features of Russell-Silver syndrome. J Ultrasound Med 1996; 15:
253–255.