Midgut Volvulus in Trisomy 21: Unveiled on Fetal Autopsy
Somya Srivastava, Shubha R Phadke Department of Medical Genetics, Sanjay Gandhi Post Graduate Institute of Medical Science, Lucknow, India Correspondence to: Dr Shubha R PhadkeEmail:shubharaophadke@gmail.com
1 Abstract
Midgut volvulus is a rare developmental anomaly with a largely unknown etiology that is challenging to diagnose
antenatally in the second trimester. The objective of this case report is to describe a rare case of midgut volvulus
associated with trisomy 21. Amniocentesis was done in a 19-week fetus with severe ventriculomegaly, hypoplastic
cerebellum, echogenic bowel, and growth restriction to rule out chromosomal anomalies. The couple opted to
terminate the pregnancy in view of the severity of the anomalies. The fetal autopsy revealed a characteristic
whirlpool appearance of midgut volvulus, and the karyotype was suggestive of trisomy 21. This is the second
reported case of midgut volvulus associated with trisomy 21 where ultrasound was not specific for this
anomaly and the gut loops were coiled in a distinctive whirlpool pattern detected incidentally on fetal
autopsy.
Down syndrome is the most common numerical chromosomal abnormality with an incidence of 1 in 850 live births and is
characterized by intellectual disability, dysmorphism and congenital malformations (Al-Nbaheen et al., 2018). Anomalies
of the gastrointestinal tract make up 5-7% of all congenital malformations and these are due to atresia or stenosis (Morris
et al., 2014). In the present case report, we describe a rare case of midgut volvulus without atresia which was incidentally
discovered in a fetus with trisomy 21.
3 Patient Details
A 29-year-old second gravida (G2A1) was referred at 19 weeks 1 day (19 weeks 6 days as per the first trimester dating
scan done at 6 weeks 1 day) of gestation in view of ventriculomegaly and short long bones in the fetus. The couple were
married non consanguineously, and the pregnancy was conceived spontaneously after one previous spontaneous abortion
in the first trimester. In the present pregnancy, the first trimester was uneventful. Aneuploidy screening was not done. On
ultrasonographic evaluation, diameters of atria of both lateral ventricles of the brain were more than 15 mm, suggestive of
severe ventriculomegaly along with hypoplastic cerebellum (cerebellar diameter - 17.2 mm; -2.2 SD for 19 weeks of
gestation). The bowel was slightly echogenic. Growth parameters and measurements of all long bones fell
below -3 SD (corresponding to 16 weeks of gestation) suggestive of potential growth restriction in the fetus.
No other soft marker or malformation was noted. A chromosomal etiology was suspected, and the couple
opted for amniocentesis for fetal karyotype, after counselling. In view of severity of the anomalies and poor
prognosis for growth and survival, the couple decided to terminate the pregnancy and submitted the fetus for
autopsy.
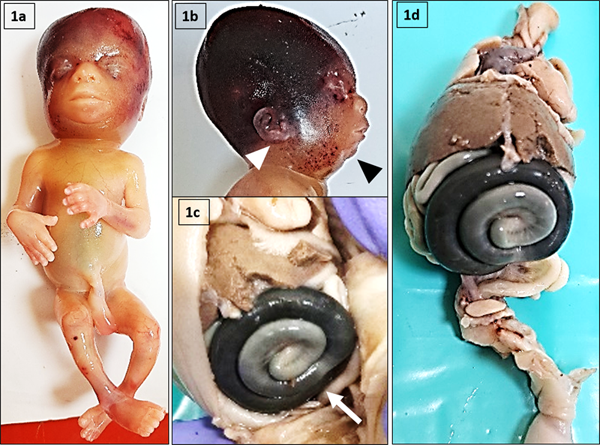
Figure 1: Images of fetal autopsy. 1a: Front profile of the fetus. 1b: Side profile of the face with white pointer
towards the low set ears and the black pointer showing the retrognathia. 1c: White arrow pointing towards the
characteristic whirlpool coiling of the midgut in situ. 1d: Internal examination of the fetal organs with the midgut
volvulus.
On external examination, the fetus was female with subcutaneous edema below the chin and lower jaw extending to
the rest of the body. Slight retrognathia and low set ears were noted in the face with intact lips and palate (Figure 1aand b). Both upper and lower limbs were devoid of any abnormality with no anorectal malformation. The cord had
three vessels. The anthropometric measurements and fetal weight fell below the 5th centile for gestational
age of 19 weeks and were indicative of growth restriction in the fetus. Internal examination of the brain
confirmed the presence of ventriculomegaly and hypoplastic cerebellum. On opening the abdomen, loops
of dilated gut were coiled in a characteristic whirlpool pattern suggestive of volvulus (Figure 1c andd). No evidence of atresia or stenosis were found on examination of the midgut. No malformation was
noted in the esophagus, trachea, lungs, and heart with an intact diaphragm. Remainder of the abdomen
and pelvic organs were unremarkable with normal histopathology. Fetal karyotype revealed free trisomy
21.
4 Discussion
Association of midgut volvulus with trisomy 21 is extremely rare. Midgut volvulus is seen in 3.9/ 10,000 live births and
can be picked up antenatally in the third trimester by various ultrasound findings of which dilated stomach and bowel,
polyhydramnios and whirlpool sign are the most frequent (Schulman et al., 1993; Shen et al., 2022). Review of videos of
prenatal ultrasonography done in our case did not reveal anything other than echogenic bowel around the
umbilicus suggesting that at early gestation the whirlpool sign may not be obvious on ultrasonography.
Echogenic bowel has been reported in 11.4% cases at a median gestational age of 31 weeks (Shen et al.,
2022).
The most common cause of midgut volvulus is intestinal malrotation. Other rare associations include intestinal atresia
and duplication, cystic fibrosis, and segmental mesenteric defect (Shen et al., 2022). Only a single case series with 11 cases
reported one fetus with trisomy 21 (Yang et al., 2022).
This is the second reported case of midgut volvulus seen with trisomy 21. Such findings can be missed in the second
trimester anomaly scan. In our case it was detected incidentally at fetal autopsy, reiterating the importance of doing a
systematic fetal autopsy in uncovering rare developmental anomalies.
Acknowledgements: The authors are thankful to the patient and her family for their consent.
Conflict of interest: None
References
1. Al-Nbaheen MS, et al. Analysis of Downs syndrome with molecular techniques for future diagnoses. Saudi
J Biol Sci.2018; 25(03): 558–562.
2. Morris JK, et al. Major congenital anomalies in babies born with Down syndrome: A EUROCAT
population-based registry study. Am J Med Genet. 2014; 164(12): 2979-2986.
3. Schulman J, et al. Surveillance for and comparison of birth defect prevalences in two geographic
areas--United States, 1983-88. MMWR CDC Surveill Summ. 1993; 42(1): 1-7.
4. Shen AW, et al. Prenatal imaging features and perinatal outcomes of foetal volvulus–A literature review.
Prenat Diagn. 2022; 42(2): 192-200.
5. Yang L, et al. Evaluation of ultrasonography in fetal intestinal malrotation with midgut volvulus.
Ginekologia Polska. 2022; 93(4): 296-301.